Rinoplastica chiusa
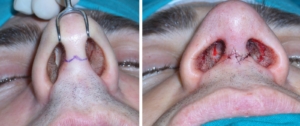
Fin dagli albori della chirurgia nasale per correggere i più diversi problemi funzionali ed estetici è stato impiegato un approccio chiuso al setto e alla piramide nasale, attraverso incisioni all’interno delle fosse nasali.
La minor invasività, la capacità di “sentire” tra le proprie dita le strutture osteocartilaginee nasali e di immaginarne la loro correzione anatomica hanno reso in passato la rinoplastica con approccio chiuso uno degli interventi più affascinanti e difficili della chirurgia estetica facciale.
I risultati ottenuti con questo approccio sono stati soddisfacenti e continuano ad esserlo anche oggi se vengono rispettate alcune indicazioni. Infatti, nel caso di presenza di “gobba” del dorso nasale associata a deviazione del setto nasale e ipertrofia dei turbinati la rinoplastica chiusa offre la possibilità di ottenere ottimi risultati con una veloce e precisa esecuzione. Viceversa, significative alterazioni della punta nasale che necessitano di sofisticate procedure di rimodellamento, se trattate con l’approccio chiuso, sono esposte al rischio di asimmetrie postoperatorie. Sono convinto anche che altri limiti dell’approccio chiuso sono presenti nelle rinoplastiche secondarie laddove un’ampia esposizione delle regioni anatomiche, come con l’approccio aperto, può essere la base per ottenere un pieno successo.